Samwise, once again, was first to spot this video. Initially there was some confusion as to whether it was recent or from last fall (2018), but Lucas, who watched the whole thing through, observed that he cited the pig study which was published two months ago. This presentation, made at Grand Rounds at NYU, was given in May this year, likely May 8th:
Link to Sam Parnia Grand Rounds May 2019
Now that I have had a chance to watch the entire video there are some very noteworthy points to make, in particular regarding the current status of the AWARE II study and a complete bombshell of a revelation which I will get to a bit later.
Firstly his presentation is a great review of the history and current state of resuscitation medicine, the area of expertise that Dr Parnia focuses most of his research work on. In particularly he spends time discussing the definition of death. Historically it was when the heart had stopped, there was no breathing and the pupils were fixed and dilated. With the advent of CPR in the 1950s this changed to about 5-10 minutes after the heart had stopped and CPR administered without the heart restarting. However, now it is clear that brain cells, the ones that will have the most significant impact on quality of life after resuscitation, could remain viable for many hours after “death” depending on the type of interventions administered from lowering body temperature to injecting magnesium. This is the area of medical research that Dr Parnia is devoting his greatest energy, and is already producing information that will help extend the period which a body remains viable after cardiac arrest. Bravo Dr Parnia, and we condone you for this great work. However, that is not the thing that gets us most excited on this blog/forum. So if you don’t want to learn all about that, fast forward to about 45 mins in when he starts talking about consciousness and death.
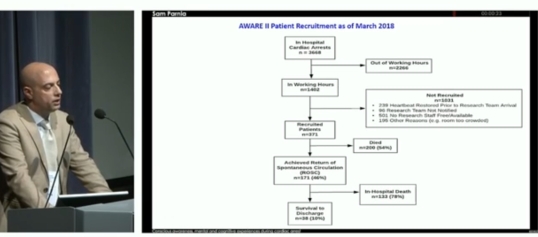
In this section he summarizes the findings of the AWARE I study, detailing the case of the man who had consciousness for 5 minutes and whose account was validated by attending Health Care Professionals (but not by the all important cards). That’s old news for us. He then mentions some of the materialist explanations of consciousness in general without getting into the details, and then the money slide:
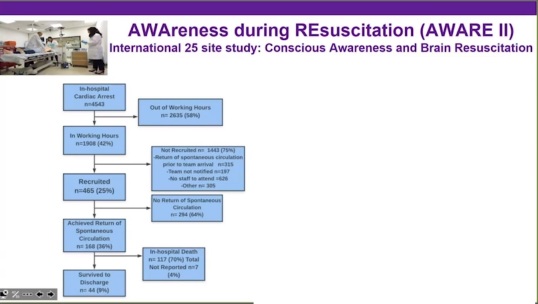
This, according to Dr Parnia, is the enrollment status of AWARE II from April 2019. My first reaction was surprise that there had been so few new cases of patients surviving to discharge. In the presentation last year in which he showed data from March 2018, 38 patients had survived to discharge, this meant only 6 new cases. Then I started to look at the numbers more closely. Firstly the math is wrong. If you subtract the number who did not have return of spontaneous circulation (ROSC) from the total number recruited, you get 171 not 168. Big deal you say, well 171 happens to be the same number that had achieved ROSC on his slide from March 2018. Something fishy is going on. Either a lot more (all) patients are dying before discharge since March 2018, or they need to get a new statistician, or something else. It just doesn’t make any sense.
Then he threw this bombshell in:

He casually stated that 10% of the patients who had a CA experienced seizure or seizure like EEG activity before ROSC. This is of course a potentially massive finding and contradicts much of what has been said before about NDEs. However, there is one key omission. There is no data on this slide showing numbers of patients who have an NDE, and even more importantly, there is no mention of correlation between reports of NDEs and this EEG activity. It is possibly the biggest teaser he has ever lobbed out to the NDE community.
Finally, Dr Parnia was scheduled to give another Grand rounds presentation focusing solely on consciousness during CA later in May. Maybe he shed more light on this discovery and managed to get the correct numbers on his slide…we won’t know until it is posted on the NYU site…Samwise will no doubt be the first to spot it.
Of course the skeptics will leap on the EEG activity, but until it is matched with reports of NDEs it is meaningless, and even then may be open to subjective interpretation. It is certainly hugely thought provoking, and at the same time frustrating until we learn more.