Lipstick on a tripping pig
After months of promising, I am finally posting this article about Psychedelic’s and NDEs. The reason that I have been kicking it into the long grass is twofold. Firstly, I always have seen and still see, data from psychedelic trips as inconsequential in terms of challenging the validity of NDEs, as you will see, and secondly there is a lot of data to review, although I have decided to focus on one paper by Timmermann from 2018, and the 2022 Parnia consensus response, and some of his invective from his book Lucid Dying.
Interestingly I may have been in a position where I would not have been allowed to write about this. Last December I was in discussions around joining a company who were in the pre-launch phase for a psilocybin derivative for treating depression as their European medical scientific lead. I had reviewed the literature and was in two minds about the risk benefit ratio of the drug, and a little frustrated by the complete lack of reporting of “subjective” effects from the studies as I suspect the perceived nature of the subjective effects might actually have had an impact on outcomes such as suicidality. No matter, I didn’t get the position (good job as the recent FDA advisory committee came out against deploying psychedelics in healthcare at this stage).
Now on to the subject. The paper that I focus on and is of most relevance is the one by Timmermann et al published in Frontiers in Psychology, not a premier academic journal. In this paper 13 patients took DMT and were given the standard NDE questionnaire afterwards. This was compared with a baseline questionnaire reflecting their non-“tripping” state, and with matched controls of people who had “authentic NDEs”.
One very important point to consider here is the fact that only 13 patients took part and they were selected through “word of mouth”. Ultimately, in my view, anyone volunteering through “word of mouth” recommendations to participate in a study taking DMT has a certain level of baseline “abnormality” that sets them apart from the normal population. Also using such a small number of patients makes it of low value in terms of the “meaningfulness” of any results. In truth, the study lacks any credibility at the outset because of these two points and would exclude it from a serious peer-reviewed journal due to this, but let’s car park that and consider what it says.
This is the key finding:
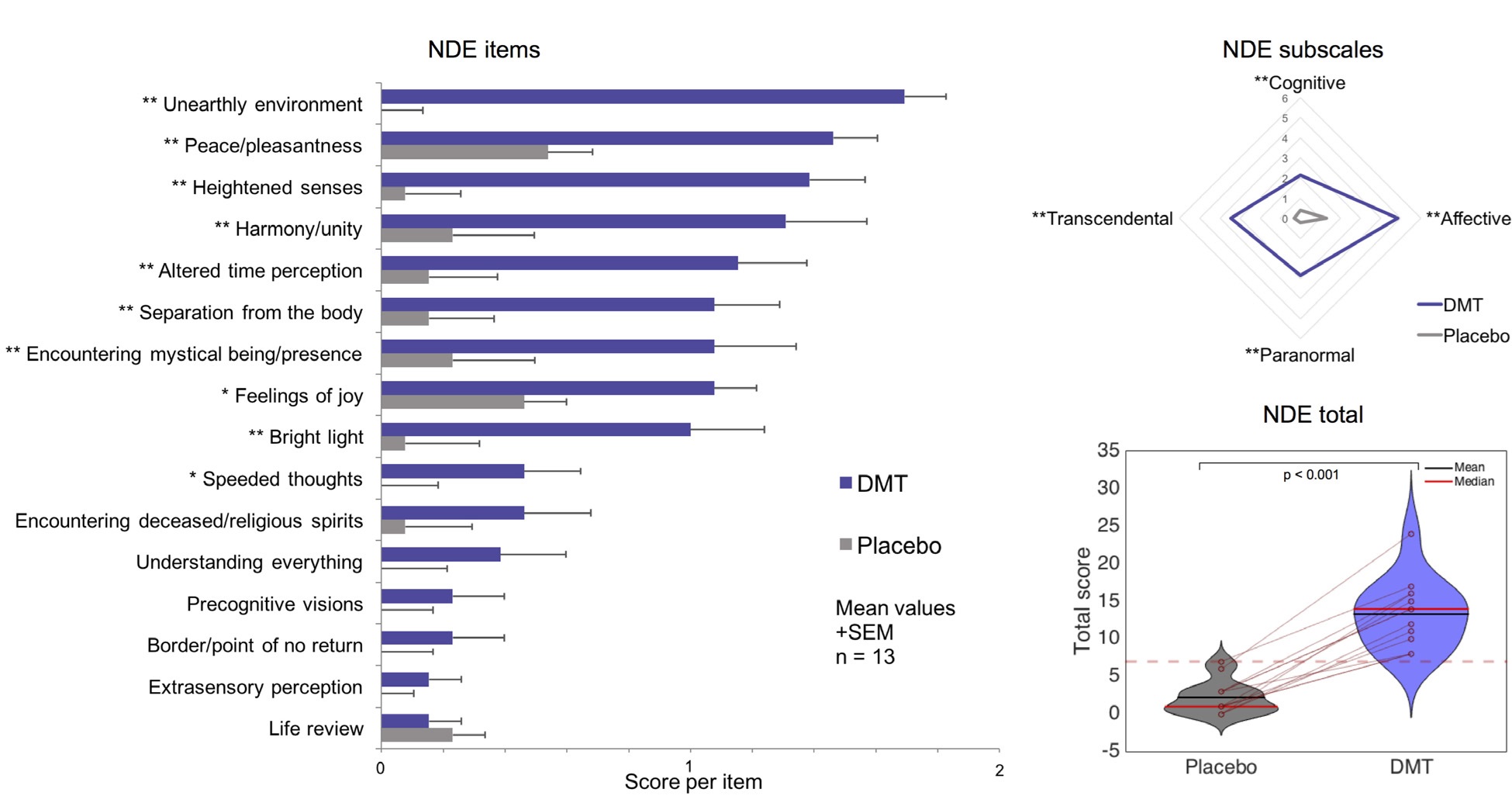
“All participants scored above the conventional cutoff (above or equal to 7) for a (DMT-induced) near-death (type) experience (Greyson, 1983). One of the 13 participants had a total score of 7 following placebo.”
The fact that one patient out of the thirteen reported an experience of greater than 7 on the NDE scale on placebo is very pertinent and speaks to the patient selection criteria…to be polite, they were probably not a representative selection of “normal” people.
Below is a graphic of the breakdown of scores for the patients on placebo vs the same group of patients on DMT:
Now here I am going to depart to some anecdotal experience. I would never admit to taking illegal substances, but I may know someone extremely well…cough cough…who went through a period when they were at University a long while ago and spent about six months consuming a lot of weed. One particular batch of weed that this friend…cough cough…had must have been spiked as he went on a massive trip. In this trip he became a wolf in another world. He was still aware of the fact that he was lying on the floor of his bedsit in Southampton, but at the same time was having this “out of body” experience, with heightened senses – time seemed to slow right down – in another world (unearthly environment), and there was even some religious symbolism…probably a 7-10 on the NDE scale.
That is the point about the above graphic. This person…cough cough…knew this was not an NDE and yet would have scored over 7 on the NDE scale, and this person…cough cough…was not someone crazy enough to volunteer for a study in psychedelics, and as a matter of fact never bought weed from that supplier again.
In this study, which is probably the most relevant of its kind, they show that DMT creates an experience that scores the same on the NDE scale as authentic NDEs. However, as this person I knew very well has shown you can have an experience that is not an NDE but scores like one. This says more about the way that NDEs are scored than the value of any conclusions you can draw from this study with respect to psychedelics creating NDE-like experiences. To the author’s credit, this is somewhat recognized:
“It is important to acknowledge that the phenomenology of NDEs is still a matter of some investigation.”
This is why the 2022 consensus paper has some value as it seeks to more precisely define the different domains of experience. In that paper Parnia has the following to say in his section on psychedelics:
“Another major contributing factor that enables some to argue that drug-induced states are similar to so-called NDE involves the misuse of research scales that were developed for the specific study of so-called NDEs in non-context-specific circumstances, even though these are not designed for, nor are they sensitive or specific enough to distinguish a classical NDE from other experiences.”
In other words, the original Greyson scale was designed specifically for NDEs and not for other experiences so using this scale to look at DMT trips makes the findings less relevant.
Timmermann also cites a paper by another NDE investigator from the sceptic camp, Martial. He says that her work showed “that the temporal sequence of events unfolding during an NDE is highly variable between people and no prototypical sequence was identifiable.” This directly contradicts the narrative arc described in the consensus paper. However, on closer inspection of the Martial paper, while there is some heterogeneity in the order of some aspects of NDEs, the suggestion that there is no prototypical sequence is not an accurate conclusion to draw. I may review this paper at another time, but there are confounding factors in the paper to consider such as the fact that not everyone experiences all the elements (she does go a little way to addressing this by looking at reports which contained all of 4 specific common elements but the conclusions are the same for me). However, when you look at the highest percentage of experience reported at sequential timepoints T1-7, you get the following sequence:
T1-OBE>T2-feeling of peace>T3seeing a bright light>T4encountering people/spirits> (T5&6) coming to a border/boundary >returning to body.
This is very much in line with the narrative arc. You could argue that because they don’t all appear at the same time point there is heterogeneity, but in reality that heterogeneity lies in the fact that not everyone reports all the elements, and that some elements are not “time-critical” e.g. feeling of peace. Ones that are, such as OBE and return to the body, occur exactly where you would expect in the vast majority of those who report these elements. This points to Timmermann’s “confirmation bias”.
Parnia seems to have taken a leaf from my book when it comes to using pejorative terms when describing other people’s work. In Lucid Dying he says the following:
“Dr Timmerman’s claim was just another example of putting lipstick on a pig.”
Quite.
However, given that Parnia uses outrageous confirmation bias in the consensus paper regarding negative experiences, something I discuss in my soon to be published book in much greater detail, I will use my own cliché “pot calling the kettle black”.
All fun and games, and if Sam Parnia ever reads this blog, he will know that we all love him here and will hopefully take our criticism in a friendly way. What he does do an excellent job of in his 2022 paper is to go into a detailed analysis of the descriptions of psychedelic induced experiences vs NDEs and reveals how different they are in reality.
Ultimately though I regard all of this as a storm in teacup – the main reason why I have struggled to spend 3 hours on a day off prior to now to cover it.
This is because:
- There is not a single veridical OBE validated by an accredited HCP who is prepared to go on the record from a psychedelic “NDE-like” experience. As we know from historical accounts, and the excellent work or Titus Rivas in The Self Does Not Die, there are hundreds if not thousands of these for authentic NDEs that defy natural explanation. In sum, these are incontrovertible proof of the validity of OBEs and NDEs.
- If there were veridical OBEs in a DMT experience, so what? All this would prove is that psychedelic drugs can cause the consciousness to dissociate from the brain thereby proving that the consciousness is either independent of the brain, or that the brain is able to project a version of the consciousness beyond its physical confines and observe things that are naturally impossible to observe – mmm.
Now I know that the likes of Timmermann approach this from the other way round to the way I suggest that they do, namely that they try to infer that NDEs are just a physiological phenomenon induced by neurotransmitters like DMT trips, and not that DMT trips are like NDEs. This is the reductionist approach, but whichever way round you look at it, the similarities are superficial and do not stand up to scrutiny – the pig is most definitely wearing make-up.
Ultimately my highly speculative view of psychedelics, and while we are on this (and I may do separate posts on these at some point), other NDE-like experiences reported due to syncope or REM intrusions etc, is that they possibly disrupt the consciousness in a way that momentarily causes it to “wobble” within it’s physical confines. This speaks to Parnia’s disinhibition hypothesis (Eduardo – shush) and the idea that there is a physiological mechanism behind the consciousness “packing its bags and leaving” that may be facilitated by certain neurotransmitters. This is highly speculative, but maybe DMT, epileptic fits, syncope etc disrupt the tethers that normally keep the consciousness in place.
Hope you enjoyed. If you did please buy one of my books or buy me a coffee if you haven’t already,

https://academic.oup.com/nc/article/2024/1/niae033/7745969
They actually published a new study in the last week of people who took substances and also had ndes. It indicates similarities and differences.
LikeLike
Again, highly suspect recruitment methods, and did these patients have a CA? None of that is clear. There is nothing in this new study that adds to what they previously said in reality. They are making lots of noise but saying nothing.
LikeLike
The study exemplifies my point that we are looking at it from opposing worldviews. They are trying to prove a reductionist interpretation that NDEs are just a result of neurotransmitters by saying that there is a lot of overlap with PEs (using their highly selective instruments). They just completely ignore the fact that OBEs in NDEs have been proven real, and therefore they need to look at it the other way round, the way we look at it…can PEs produce a similar experience.
LikeLiked by 1 person
the interesting bit for me is the part whereby the obe element within ndes are greater than anything in comparison to tbat of substance relates experiences. I can speculative imagine the filter theory enabling this.
LikeLiked by 1 person
Taking drugs to hallucinate is different then actually having an experience. Afterlife experiences are caused by lack of blood flow to the brain and absence of brain activity. You can’t hallucinate if your brain is not consciously functioning and having a lack of flow to it. What causes NDEs isn’t clear but there is no consciousness flow to the brain during an NDE which is what causes people to suspect it’s an outlying factor that is separate from the brain.
LikeLike
Ben, I agree that Parnia did a very good job in his “Consensus” in distinguishing psychedelic experiences from NDEs.
Regarding his theory of disinhibition he mentions “brain disinhibition and activation of latent pathways”, and in various media he speaks of “activation of inactive parts of the brain”. I think it would have been more accurate to say: “disinhibition of consciousness”.
LikeLiked by 1 person
If we will never see a verified obe on a peer review science papper not on bestseller?If the nde will reduce to anecdote?who can answer?
LikeLiked by 1 person
Hi Jing and welcome. Your comment is spot on, and is the big issue for the reductionists, or physicalists, or materialists…the die hard unbelievers. I agree that without a scientifically verified OBE in a peer reviewed paper these people will never believe. I also hold that even if there is was one, they would still not believe!
So will we never see a scientifically verified OBE? I do not know the answer to that question. Sam Parnia suggested in his recent book Lucid Dying that you would need 50,000 in hospital CAs to get one (In AWARE II they got just over 500 if I remember). I think that is an over estimate. Let’s do the maths using existing statistics:
If 10% of those having a CA survive till discharge (or interview), 50% of those agree to take part, 10% of those had NDEs, and 25% of those who had NDEs have OBEs in this dimension then you would need 800 in hospital CAs to have one patient survive till discharge who had an OBE where they might have observed events in this dimension.
The next bit is pure guess work i.e. how many of those who had an NDE AND an OBE would notice the iPad and make a note of the image on the screen. Let’s be super conservative and say only 10% of those would do the latter, this would mean you’d need 8,000 patients to get one hit, let’s round that up to 10k.
Now I suspect that Parnia is adding on the complication of having sufficient staff to be able to reach these in-hospital CAs with the modified crash cart, and so when he is using the number 50,000 he is talking about the total number of in hospital CAs, not just those where the crash cart arrived in time.
If there was a huge desire by humanity to answer this question, and get a scientifically verified hit, then we could do it in a year…but there isn’t. However, I believe the reductionists, led by Martial are designing a study to try to disprove OBEs are real by using the stats in their favour. Be interesting to see how that one turns out, also incredibly easy to shred it to pieces if the numbers of “participants” is low, but that won’t stop them trying to bang their drum along with their media sympathisers in the Guardian, NYT etc. If they actually had 10,000 in hospital CAs where the crash cart arrived, and there were claims of 10 OBEs occurring in this dimension, but not a single one observed on the iPad, then they might have a point. But they won’t do that, they will probably use data from a few hundred to say they have proven their hypothesis, or at least disproven the hypothesis that OBEs are real.
On the subject of non-scientifically verified OBEs, I understand your sentiment when it comes to “best seller” books. (Lord knows I’ve tried, but with no luck so far 🙂 ). However, if you look at the Self Does Not Die, the vast majority of the veridical OBEs in that book never became the topic of best sellers in their own right, and many were based on reports by highly respected medical professionals who make more money in a year than most authors make in a lifetime from writing (which is why I need a day job!). Surgeons in the US often earn upward of $500,000 a year, why on earth would they risk their reputations and thereby their careers by attaching their name to something that is regarded as “wacko” unless they were absolutely certain that what they witnessed was not explicable by science? Given the large number of these, and the credibility of the people involved, I find this compelling.
LikeLiked by 1 person
That’s why I said in a previous message. People just reject the prospect of any form of eternal life. If humanity is immortal and they discover death is an illusion and eternal life is the truth they will naturally do anything to deny it even if the evidence towards the contrary is right in front of their face. The prospect of immortality scares humans so they will try to deny it rather then accept it and fabricate excuses to make it seem like they are right. These are the type of people who if you showed them evidence of verified NDE/OOBE they will just give you a weird look and think you are crazy and go on some excuse that it’s the brain even though evidence says otherwise. I for one like life so I embrace the thought of an eternal existence.
LikeLiked by 1 person
Well put TS. I am very excited about the prospect of eternal life and all that it may hold. I almost look forward to death because of it! And yes, those who are of a different kind of thinking just cannot see things that way, and unless their minds are shaken up, never will.
I was watching a discussion between Ayaan Hirsi Ali and Richard Dawkins recently. Ali has travelled the road from Islam, through atheism, when her and Dawkins became buddies, to Christianity. She said that Dawkins and she were now on different planes of thinking. If you think there is nothing, then nothing is possible, but if you think there is “something” then everything becomes possible. It was a really elegant way of showing why atheists cannot even contemplate the things we understand to be real.
My next non-fiction book which is going in for copy editing next week, delves into this subject a lot more. Release will be early November…before that I will be releasing a novel in 12 days time that also explores this in a format of an adventure.
LikeLike
I hope,the verified obe will not only mentioned by bestseller book.I hope human won’t have to make a only one choice from science and spirituality.I hope the “war” betwen the science and religion will be reconciled.But I’m too weak to change anything.Maybe we still have hope.But it look like pretty remote.
LikeLiked by 1 person
This is only one front on that “war” Peter. The subject of the origin of life is much more clear cut. In my book DNA: The Elephant in the Lab, available on Amazon (remember, my real name is Orson Wedgwood) I show that science disproves the “belief” that life could have started by natural processes and that there is evidence to support that it was initiated by an intelligent being (I am not referring to evolution, but specifically to the origin of the DNA – Protein system). My background is that of being a Ph.D. organic chemist who worked in the lab on nucleic acids and Amino acids to disrupt viral replication of RNA and production of proteins. In my career after my Ph.D. I also worked in areas of medicine which focused on disrupting DNA/RNA replication and protein synthesis in a number of diseases, so I am a genuine expert with credentials in this field.
However, I do believe that there is “supposed” to be a balance between evidence supporting the existence of God and evidence against this, and that this is possibly intentional. I go into that in more detail in my upcoming book.
LikeLiked by 1 person
Complementing Ben’s position ….
A Reflection
Applying common sense to NDE research.
Rejecting anecdotal evidence?
It is true that most evidence for truthful perceptions during the OBE part of a NDE is anecdotal.
But, for sceptics this evidence simply does not exist. Never mind that anecdotes number in the hundreds: “The plural of anecdotes is not data,” they say. As thinkers and scholars have pointed out, not taking anecdotal information into account when trying to construct a picture of reality is a major intellectual and methodological mistake. Anecdotes (the stories people tell) are the basis of our legal system, for example. Imagine what court proceedings would be like if we automatically ignored the testimony of witnesses in court. Imagine what a GP’s job would be like if he or she had to automatically classify as “inaccurate, unreliable, faulty” anything a patient says during a consultation. And the fact that I had coffee in the kitchen this morning with my wife and one of our two cats has not appeared in a peer-reviewed scientific journal. Nevertheless, it is a fact.
Piero Calvi-Paris
LikeLiked by 1 person
There is also differences in quality of anecdotal accounts. My father had an NDE when he was a child and had an OBE. Him telling me that is for me an excellent anecdotal account, but outside of my family, it is poor.
A patient who tells a doctor he saw a quarter on top of a 7 foot high cabinet, and the doctor then recovers that quarter, and goes on the record stating what happened is, in my view, as close to a scientifically verified account as you can get.
Then if you have dozens, or in the case of the Self Does Not Die, hundreds of HCP verified accounts, which have been meticulously compiled and documented by the authors, then the weight of evidence is absolutely overwhelming. To question the validity of this is actually insanity. It is proven.
LikeLiked by 1 person
Kudos to Titus Rivus and his co-authors on a wonderful compilation. I’ve bought copies and gave them away to family members as its such an important book.
LikeLiked by 1 person
I agree. It took me a while to read it, but then realised how dumb I had been not buying it sooner! Really really important piece of work since it amounts to proof beyond any reasonable doubt that OBEs in NDEs are real. To question that is totally bonkers.
LikeLike
true. This week i learned about an ex minister of my country, a very prominent politician and respectful lawyer, had an nde last year when in hospital with a severe desease. He said on a tv interview that now he has 100% sure about life after death. He would not have exposed himself if he wasnt 100% sure of what he experienced.
LikeLiked by 1 person
I agree. I’ve been debating this topic with someone on Facebook. There is no getting through to him. Some people just have to experience it for themselves.
LikeLiked by 1 person
I just read two good books on NDES and psi phenomenon. One is called Do We Survive Our Biological Death the other is called An Urgent Message for Humanity.
LikeLiked by 2 people
Anyone know of any new interviews with Sam Parnia. His book Lucid dying just came out. If anyone knows of any new interviews, please let me know. Thanks
LikeLike
I’ve read several articles by neurosuregons explaining that the gland producing the DMT can’t produce enough for a DMT trip when we are dying and that it is too slow to produce enough DMT within seconds to cause such a hardcore trip that would make you hallucinate that strongly (NDE like) so I don’t even understand why this dude made that study anyways because it’s useless. Our gland that produces the DMT is _physically_ *unable* to produce this kind of a trip amount.
LikeLiked by 1 person
Here is an interesting read btw…
https://www.healthline.com/health/pineal-gland-dmt#production
“Your pineal gland is tiny — like, really, really tiny. It weighs less than 0.2 grams. It would need to be able to rapidly produce 25 milligrams of DMT to cause any psychedelic effects.
To give you some perspective, the gland only produces 30 micrograms of melatonin per day.
Also, DMT is quickly broken down by monoamine oxidase (MAO) in your body, so it wouldn’t be able to naturally accumulate in your brain.”
“The most recent animal study on DMT in the pineal gland found that even after removing the pineal gland, the rat brain was still able to produce DMT in different regions.”
LikeLiked by 2 people
Terninal lucidity
Hello, sorry if its not the right post but i can’t find an other older post thst talked about this, i remember that it was re Sam Parnia book.
My question is: does terminal lucidity appears in Alzheimer desease or only in dementia cases?
This because i saw a post on Reedit that state that it doesn’t manifest when people suffers from Alzheimer. If this is true, i wonder why?
LikeLiked by 1 person
Hi Marii,
I would be very surprised if terminal lucidity was not experienced in patients with dementia due to Alzheimer’s. Alzheimer’s is largest cause of dementia in the elderly. Also the phenomenon can occur in a number of conditions in addition to dementia where damage to the brain has resulted in a patient’s ability to communicate or process information has been severely impaired e.g. stroke. There has not been a huge amount of research done on this to date, but Parnia is on the case, so hopefully he will be presenting some data before long.
LikeLike
In fact this case was in a patient with AD, so I would ignore Reddit. Unless there is a reference to a scientific journal making statements like that, it is probably garbage.
https://alz-journals.onlinelibrary.wiley.com/doi/full/10.1002/alz.12424
LikeLiked by 1 person
indeed
thank you!
LikeLike
Hi Ben. I haven’t seen this to completion (listening to it as I write this), but I thought I’d bring it to your attention.
https://youtu.be/Kg8EJyL2jsA?si=TouNWxYIi_kdv7Qw
LikeLike
The statistics are interesting, especially if viewed within the context of NDEs.
LikeLike
Mental Activity During Deep Hypothermic Circulatory Arrest – Health Research Authority (hra.nhs.uk)
It looklike is the summary of UK part of DHCA study(but I don’t know if it really conduct in UK),more detailed than nyu’s summary.Don’t know what that means.If 50 DHCA patients is true,the study will finish in not far future.I konw your attitude of DHCAstudy,Just a mention.
LikeLike
Thanks Peter. Interesting how far back the ethics approval was…2019. We know they had their first patients in NYU in 2020 despite COVID. If there were any interesting results I would have expected them to have presented or published something by now, so I suspect it was a bust.
My hope for these studies has diminished after the other study that looked at this had zero patients out of 100 who had memories. Love to be wrong.
We will see.
LikeLike
Deep Hypothermic Circulatory Arrest: A Brief History and Where It Is Going – Journal of Cardiothoracic and Vascular Anesthesia (jcvaonline.com)
In this papper,It published in 2024.they didn’t mention “the method change”,just say”Most centers have
developed protocols centered around hypothermic ranges from
18˚C to 20˚C.”
If it higher than 20˚C to 28˚C,it always called “moderate hypothermia Circulatory Arrest”(MHCA).There are a lot of Comparative experiment Between DHCA and MHCA.so I think them is different.
中度体温过低循环停止 – Google 学术搜索
In the Mauduit study,they only has 34% patient has burst suppression,it may not eough.
I’m comfirm you know it.but I don’t know Why you so determined that DHCA study will failure.
I’sorry for my tone.
LikeLiked by 1 person
I’m just used to failure now in these studies now!
LikeLike
Interesting article regarding new search on consciousness and microtubules for any who have not seen it yet.
Link: https://www.popularmechanics.com/science/a62373322/quantum-theory-of-consciousness/?utm_source=pocket-newtab-en-us
no paywall: https://archive.is/1eaEf
LikeLiked by 1 person
search = research
LikeLiked by 1 person
new research on consciousness and microtubules
https://archive.is/1eaEf
LikeLike
NDEs and dreaming relation. American Psychological Association link, recent 2024 paper https://psycnet.apa.org/fulltext/2025-09084-001.html Upshot … “those who experienced NDEs were significantly more likely to report unusual dream experiences, especially lucid dreams, precognitive dreams, and OBEs.”
LikeLiked by 1 person
Ben is your book coming out soon on NDES. If so, whats the title and when is it coming out
LikeLike
2 books are coming. A novel in 2 weeks time, and a non-fiction book about 2 weeks after that. All under my real name Orson Wedgwood 🙂
LikeLike
Hi Ben
Just wondering is it paperback or ebook or both for the 2 of thrm and which outlets will they both be sold?
thanks
Z
LikeLike
https://www.dailymail.co.uk/health/article-13907689/scientists-state-life-death-neuroscientist-experience-unbearably-intense-icy-blue-light.html
big paywall here but would love to hear thoughts from anyone able to read
LikeLike
I’m not subscribing to the Mail, it has become garbage over the past few years! Be good to have access to the article though, for sure.
LikeLike
Dr Christof Koch, a neuroscientist at the Allen Institute in Seattle, a leading brain research centre, knows a great deal about near-death experiences (NDEs) – where people report having mystical encounters after they were declared clinically dead, but then were successfully revived.
Dr Koch has spent 35 years studying consciousness: he is eminent in his field, the author of more than 350 scientific papers and many books. But he knows NDEs intimately because, four years ago, he experienced one himself during a health emergency in the early days of Covid.
‘It was utterly remarkable,’ he recalls.
‘I saw a singularity of overwhelming brightness and felt terror and ecstasy.
‘Nothing else – no body, no Christof, no self, no identity whatsoever. But also no world and no passage of time. Nothing except for the icy light,’ he said recently.
‘Nothing was left but a non-self… it [this ‘non-self’ he’d become] didn’t want anything, expect anything, think anything, remember anything, dread anything. But it [the non-self] experiences… It saw a cold, white light of unbearable intensity, unable to conceive of looking away, as there was no ‘away from’.’
There was ‘no smell, no pleasure, no pain’, just ‘a timeless universe convulsed to a blazing, icy light’.
Dr Koch, 67, says this experience has marked him for life – not least because he says he no longer has any fear of death (which is ‘not uncommon in people who have undergone an NDE’). It has also made him a unique figure in an emerging new era of research into dying and death.
Death remains one of life’s greatest mysteries. But new scientific investigations into the bizarre medical phenomena that can arise when we approach death, and even afterwards, may start to unravel it (or make it even more mysterious, as we shall see).
This could help researchers develop new ways to cure debilitating illnesses such as cardiovascular disease and cystic fibrosis – and improve vastly resuscitation techniques and the care of the dying – within just five to ten years, according to some experts.
The latest discovery in this field of death-science reveals something that sounds quite spooky, but which may soon offer revolutionary lifesaving cures: our own human cells can grow into microscopic new creatures after we die.
It’s not quite the after-life as we might have imagined it, but nonetheless it is a discovery with extraordinary implications.
Scientists are also focusing on an astonishing phenomenon called ‘terminal lucidity’ – where terminally ill patients who have long been unconscious suddenly rally into life and communicate happily with staff and visitors, shortly before dying.
And then there is the better known, but just as mysterious, near-death experience.
Such phenomena have traditionally been dismissed by doctors and scientists as just unaccountably weird, or simply invented or imagined. Now leading experts are starting to take them very seriously.
All these strange phenomena raise the question whether the apparently solid boundaries between life and death are far more porous than modern science currently holds.
Renewed debate about what happens to us when we die has been sparked by a recent report by a group of eminent biologists in the US. They argue that, as well as ‘alive’ and ‘dead’, there actually exists another condition called the ‘third state’ – which ‘lies beyond the traditional boundaries of life and death’.
The ‘third state’ is a term coined by Peter Noble, a professor of microbiology at the University of Alabama at Birmingham in the US, and one of the authors of the report (published in the Physiology Journal).
As he explained to Good Health, in this state after we are clinically dead, our bodies’ individual cells can survive and reform themselves into new, multi-cell life forms that can replicate themselves – effectively breeding new life after death – and may even be able to repair other human tissues.
He says this intriguing ability of cells to survive Lazarus-like from dead creatures was first demonstrated three years ago by Michael Levin, a professor of biology at Tufts University in the US.
‘He found that skin cells extracted from deceased frog tissue were able to adapt to the new conditions of a Petri dish, spontaneously reorganising themselves into multi-cellular organisms that could even replicate themselves,’ explains Professor Noble.
‘Not only that, these new creatures [called ‘xenobots’], could do much more than simply be skin cells – they used their cilia [small, hair-like structures] to move through their surroundings, whereas in a living frog, cilia are typically used to move mucus around the creature’s slimy skin.’
If that were not astonishing enough, Professor Noble says that Professor Levin’s latest research, published in January in the journal Advanced Science, suggests that cells taken from a human windpipe also reorganised themselves into multicellular creatures, called ‘anthrobots’.
And when these anthrobots were placed in a Petri dish with damaged nerve tissue, they attempted to repair the nerves.
How could individual cells reinvent themselves from their previous existence in a living body? One theory is that complex animals (and ultimately, humans) evolved as single-celled creatures joined together to cooperate to create multi-cellular creatures.
This involved them giving up their autonomy to serve narrow roles within the multi-celled creature (rather like a multi-skilled craftsperson getting a job doing only one thing on a factory production line).
In reverse fashion, Professor Noble believes that when a multi-celled creature dies, their cells can revert to their previous individualistic states with all their old abilities, such as the frog cells’ swimming, and then re-form in new ways that might enable them to survive their host’s death.
‘We should not be surprised that human cells can do the same thing as ones from frogs,’ he says. ‘Who knows what can be created? Until now, we’ve never looked.’
Beyond showing that our cells are more resilient and resourceful than previously imagined, ‘these discoveries offer prospects for remarkable new treatments’, says Professor Noble.
He predicts that soon specially evolved medical anthrobots could be made from living patients’ own tissue and injected back into their bodies to perform specific tasks.
These could include repairing damaged spinal cords, clearing plaques in arteries and removing excess mucus from the airways of cystic fibrosis patients.
The anthrobots may also deliver medication, such as chemotherapy, precisely where needed.
Such advances may come sooner rather than later: ‘I think we are five to ten years away from clinical applications,’ says Professor Noble.
The fact that cells may survive clinical death may help not only create revolutionary therapies, but could also explain near-death experiences.
NDEs are triggered by major events such as a heart attack, shock or suffocation.
Studies generally suggest that more than one in ten hospital patients who recover from being clinically dead through cardiac arrest recall having an NDE.
These experiences usually share much in common, such as becoming pain-free, seeing a bright light at the end of a tunnel, meeting deceased relations, or seeing one’s life flash in front of one’s eyes.
Not all NDEs are comforting. In a 2019 study published in the journal Memory, 17 of the 123 patients who reported an NDE recounted seeing demons, visiting Hell or falling into terrifying voids.
Charlotte Martial, a neuroscientist at the University of Liège in Belgium, who co-authored the study, is now trying to verify patients’ claims about their out-of-body experiences during NDEs.
Around eight in ten people who’ve had an NDE report leaving their body, sometimes stating facts about their environment that they seemingly should not know.
To test this, Dr Martial has decorated a resuscitation room at Liege University Hospital with unexpected objects and images, some of which are hidden in places that could be viewed only from the vantage point of someone near the ceiling – she is then asking patients who report NDEs if they’d noticed anything unexpected in the room.
But what actually causes NDEs? Professor Noble’s group cites a recent study of 11 cardiac arrest patients from the UK and US who reported having near-death experiences while their brains appeared clinically dead (i.e. where the electrical activity had flatlined).
However, as the journal Resuscitation reported, when the patients finally began to revive through doctors’ resuscitation efforts, their brains’ cells had survived so well – even after up to an hour without oxygen – that they experienced sudden spikes of the sort of activity normally associated with higher mental function, such as thinking and imagining.
The patients had also had typical NDEs. One, for example, recalled, ‘I thought I heard my grandma [who had died] saying, ‘You need to go back.’ ‘
Dr Sam Parnia, an associate professor of medicine at New York University who led this study, says that it shows these patients were experiencing ‘lucid consciousness’ even though they seemed clinically dead, and that brain cells can survive and even continue to function during extended periods without oxygen.
A major implication, he says, is that ‘a lot of physicians are taught that after, say, three-to-five minutes of oxygen deprivation, the brain dies. Our study showed this is not true.’
He adds: ‘It showed that the brain may not be functioning, which is why they flatline. But if you’re able to resuscitate them appropriately, you can restore activity up to an hour later.’
Conventional medicine is writing off these patients prematurely, he argues.
‘Nobody has tried to find treatments or new ways to restart the heart or prevent brain injury. They think it’s futile.
‘Our work opens the window to developing cocktails of drugs that could be given to patients who have technically gone through death to bring them back to life again.’
But why do patients whose brains are clinically dead report mystical NDEs?
Dr Parnia’s theory is that when the dying brain flatlines, the normal ‘brakes’ come off our brain cells’ control systems –this disinhibition may then open access to ‘new dimensions of reality, including lucid recall of stored memories from early childhood to death’. But other leading investigators disagree.
Dr Koch, whose own NDE inspired his new book, Then I Am Myself The World: What Consciousness Is And How To Expand It, argues that this research doesn’t show patients were having NDEs while their brains were flatlined.
He says: ‘They could have had these memories come to them later, before they fully returned to consciousness. The patients wouldn’t be able to know when the NDEs had happened.’
Instead Dr Koch (who said ‘I hope I will never again have to undergo [another such experience] as it is utterly terrifying’) suggests that these experiences may occur as dying brains effectively have the bounds of their egos fall away, along with their sense of space and time.
In this way people undergoing an NDE experience what he calls ‘mind at large’, a form of consciousness that may pervade the entire universe.
While this may sound mystical or religious, Dr Koch believes that consciousness is a physical quality of the universe, just like magnetism, gravity or any of the forces proposed by quantum physics.
‘Therefore all this may be explained scientifically one day,’ he says. ‘But not yet. Nothing in the current laws of physics, chemistry or biology explains consciousness. Yet here we are, seeing, hearing, feeling.’
More mysterious still, perhaps, is another death-related anomaly that scientists are beginning to take seriously, called terminal lucidity.
Over the past 250 years, physicians have recorded cases of terminally ill and long unconscious patients suddenly rallying into life, communicating with medics and family, but then dying shortly afterwards.
Commonly, these patients are the least likely to rally – those who’ve suffered prolonged, irreversible brain decline as a result of meningitis, dementia, stroke or brain tumours, for instance.
Terminal lucidity incidents may also be very common. In a survey of nursing-home caregivers, 79 per cent reported they’d witnessed patients who’d been in deep comas suddenly rouse and coherently say their goodbyes before dying, reported the journal Archives of Gerontology and Geriatrics in 2010.
Some experts have suggested this might, oddly, reflect cultural values deeply ingrained over a lifetime that it’s polite to say ‘goodbye’.
But if terminal lucidity were culturally ingrained, it wouldn’t happen in very young children. Yet earlier this year, case reports from two paediatric hospitals showed that terminal lucidity can occur in children as young as two, reported the Journal of Nervous and Mental Disease.
One three-year-old girl was in end-of-life care for an autoimmune disease: one evening after a fortnight’s unresponsiveness she began talking with her parents, which they and the nurse described as ‘like a miracle’.
She talked to all of the important people in her life, spoke of her impending death, and reassured loved ones of the need not to be concerned about her. She also seemed to be communicating with people who were not visible to others.
After several hours, she asked to ‘go to bed’ and she returned to her comatose state.
After 48 hours, she died in her parents’ arms.
‘Children so young would not be expected to have the cultural conditioning or developmental capacity to understand the concepts of death and dying, nor be aware of the emotional impact of their impending death upon their parents,’ researchers said.
Chris Roe, a professor of psychology at the University of Northampton and one of the report’s co-authors, told Good Health that terminal lucidity has clear parallels with NDEs.
‘But there is an extra layer – it involves people whose conditions are usually regarded as irreversibly deteriorated,’ he says. ‘It is very difficult to imagine how they could suddenly and briefly get better.
‘People often think that they are miracle recoveries but they typically are not. Instead, they are the precursor to death.’
Such experiences can be a double-edged sword for loved ones, adds Professor Roe.
‘With dying children it can be especially heart-rending,’ he says. ‘But, conversely, if you have a child who dies with grace and serenity, it can be a considerable comfort.
‘After the initial shock of witnessing what they’ve seen, parents are usually extremely glad about what happened.’
Beyond examining the emotional experiences, Professor Roe says that scientists have a duty to understand terminal lucidity and its biological implications.
‘We need to study a lot more cases to verify this as a medical condition and explore what underlies it,’ he says.
‘We are very open to the idea that we can explain it biologically or neurologically. Nevertheless its explanation may lay beyond the realms of current science.’
He adds: ‘We believe that terminal lucidity is not rare – many nurses tell us they have seen such things often, though they won’t discuss it with medical colleagues for fear of being dismissed as silly.’
Professor Noble adds: ‘I’ve lost count of the number of times that people have reacted by calling this work ‘Frankenstein science’. But I don’t mind, because it sparks public interest in what’s being done here to explore something mysterious – something that could prove vitally important to our lives.’
LikeLike
Thanks Pablo…I am normally against people cutting a pasting whole article, but not in this instance 🙂 I will in fact create a brief post on this.
LikeLike